Full transcript with images below – or watch as a video with subtitles.
The ways in which we relate to work are often shaped by our training experiences, and this is particularly true in medical education.
Today Paula is talking to Dr Louise Younie, GP and Clinical Reader in Medical Education at Queen Mary University of London.
The pair discuss how Louise draws on creative enquiry and the concept of flourishing to support medical students to embrace their vulnerability, find their voice, and value their humanity.
You can connect with Louise on Twitter @LouiseYounie, or via her website. Also see her book chapter What Does Creative Enquiry Have to Contribute to Flourishing in Medical Education? and paper on vulnerable leadership.
I’d love to connect with you so come and find me on LinkedIn, Twitter or Facebook.
Sign up to my weekly newsletter here to get updates about the podcast as well as psychology tips and insights direct to your inbox.
Follow and subscribe so you don’t miss an episode!
Transcript
Paula: Hi, I’m Dr. Paula Redmond, a clinical psychologist and you are listening to the When Work Hurts Podcast. On this show, I want to explore the stories behind the statistics of the mental health crisis facing healthcare professionals today, and to provide hope for a way out through compassion, connection and creativity. Join me as I talk to inspiring clinicians and thought leaders in healthcare about their unique insights and learn how we can support ourselves and each other when work hurts.
[music]
The ways in which we relate to work are often shaped by our training experiences and this is particularly true in medical education. My guest this week is Dr. Louise Younie, Clinical Reader in Medical Education at Queen Mary University of London. In this episode, she tells me about how she draws on the concepts of flourishing and creative enquiry with medical students. We began by discussing some of the challenges of medical training.
Louise: I have my own experiences from quite a long time ago and then the students that I meet and the stories that they tell me within the education setting, not within the pastoral setting. It’s an incredibly competitive process to get in and the competition remains. I was just chatting to a student today saying that actually there’s a few reasons why I think it’s harder today than it was when I went through because the students are ranked.
For all their different exams that they take, they get a little score, a number score. Through the whole of those five years, it makes you incredibly competitive, and those scores matter because it defines whether you get close to your first choice of where you’ll work in the end. That sets up people somewhat potentially against each other because anyone getting a better grade than you changes your ranking. There’s a lot of pressure to learn a lot of facts and develop a lot of skills. There’s a lot of talk about becoming competent in lots of things and there’s a heavy, big timetable.
I think some of the stuff students face as well is often as quite young people coming in, they start to meet people who are suffering at quite a young age and that’s something that they may not be as well prepared for as they might because that hasn’t traditionally been a focus of medical education. The focus has traditionally been about developing future people to diagnose and treat disease, and the aspect of walking alongside people who are suffering is less well…
That whole human dimension is less well explored, articulated, developed. Sorry, just to add to that, I suppose what we do know is that there has been documented even before COVID a burnout epidemic and stress and rise in mental health challenges across both students and clinicians. In 2019, the BMA, the British Medical Association, the General Medical Council and Health Education England, all did wide-ranging surveys and into the mental health of students and clinicians, again, confirmed these findings that are concerning.
Paula: It’s interesting as well because I guess you are working in the undergraduate part of training, because, I guess one of the things that always strikes me is that training just goes on forever and these relentless pressures can be for– and it seems like decades-long that people can be in the pressures and the exams and it seems like a moving target all the time.
Louise: Yes, there’s exams, once you qualify, there are further exams. Then you’re obviously being paid and you’re working and studying for exams. I don’t even know if that’s the hardest part of it, really. I think the pressures that we’re facing in the NHS and the time pressures and the pressures of people’s needs and the resources mismatch possibly on an ongoing basis is maybe even more challenging in a way.
Paula: Do you think that comes as a shock to people when you see people at the beginning of their career as they get to grips with the reality of what it is like to be a doctor compared to what they’d hoped, what they’d thought it might be?
Louise: I think it is a shock. I think it’s hard. I was just speaking to a fourth-year medical student who works with students wanting to apply. The context of widening participation, wanting to apply to medical school, and just saying how the A-level students see it as this big rosy bubble, but that it isn’t quite when you come into medical education. I think they can obviously see and hear what’s happening in the NHS, but I think it’s only as you get closer to the end that it really starts to hit home probably, and I say that from reading some of the fifth-year student work around that.
Paula: Louise, I know you’ve got a special interest in the field of what’s called creative enquiry and human flourishing. I’d love to first of all maybe hear about how that came about for you.
Louise: When I started I went through medical school wanting to learn the facts and the skills and thought being a good doctor was knowing how to diagnose disease. It really wasn’t until I hit general practice and started, I suppose, to be on a more level playing field with patients and really started to listen to patients and they could come back if things weren’t getting better or resolved. I started encountering people suffering in all kinds of different ways and a lot of our conversations and a lot of what happened in the consultations wasn’t necessarily about a diagnosis or treatment.
There was some of that, but that was only part of it. People suffer in all kinds of different ways, what’s happening to them socially, what’s happening emotionally, existentially, as well as what’s happening to them physically, and these are all intertwined. Trying to work out what best to do in the moment with the patient sitting in front of you became like a really challenging puzzle. I suppose it’s maybe about being holistic or having wisdom and it went way beyond, it felt like my training and I felt like I didn’t necessarily have that way to traverse from my own inner world to the other persons. I was like having to find language in ways.
For example, if you meet someone with depression for the first time, we are trained to find out how you’re eating, how are you sleeping, have you thought about harming yourself, and things like that, which are all around, is it a diagnosis of depression and how bad is it? Actually, there’s all the stuff around what’s happened to you, what’s been going on, the whole story behind it.
Often I find myself saying, “Maybe you’re having a normal response to some difficult things that are happening right now.” We have those kinds of conversations, but that’s all outside of my training anyway. As I was discovering all this and the puzzle and the complexity of that, I felt like we needed to do something different in medical education. I became a lecturer at the same time as I qualified as a GP and felt like we need to create a different space, a different way of engaging with what I now call the human dimension.
I haven’t found any better ways having been at it for about 20 years than using the arts. Creative enquiry. What I mean by creative enquiry is exploring your lived experience through the arts or it can be exploring the patient’s lived experience as you perceive it through the arts. I started running both student-selected small groups with like groups of 12 students working with arts therapists and arts for health consultants.
I still run that group. I’ve got two set up for this coming academic year, nearly 20 years down the line. Also introduced it across a whole curriculum like in their GP placement, so rather than just writing a reflective essay about Mr. S who’s got diabetes and takes his medications, we invited them to engage in some creative enquiry if they wanted to as an alternative choice.
Then the students stretched that space like, we had a few poems and a few narratives of first year. Then I fed that back and explained it a bit more, and gradually they were doing sculptures and music, and actually as an educator I was learning so much both about them and the patients. Yes, that was a starting journey.
Paula: Tell us more about what creative enquiry means to you. You said it’s about exploring experience and why do you think that the creative part of that is so useful?
Louise: I don’t know if Freud actually said it, but it’s attributed to him that he said, “Wherever I go, a poet has been there before me.” There’s something about the creative process that is like a lightning rod into our stories, our narratives, our lived experience. Lived experience actually doesn’t easily find itself necessarily on a written page of prose, but actually, when we start engaging with metaphor, symbol, different languages, we can engage with some of the feelings that we felt in those moments.
We can represent things without fully nailing the colors to the mast, if you like. It actually gives us more languages to work with. It’s like becoming multilingual in reflecting on our experiences. We have got a bit of a problem with students feeling like there’s a tick-box reflective culture where you just have to write something reflective and endless reflections, but actually, to be reflective, first of all, there needs to be a safe space and we need to recognize that it’s a vulnerable thing to reflect.
If you create a safe space and then opening that door to creativity, and particularly with that group of first-year students where they were new, it gave them a choice to– this was from my doctoral research, to find their voice. Actually, the student’s voice came out in a different way. I usually have pictures to show, to explain what I mean a bit better, but there’s one example of a student who did an image of a slumping lady and a bit of a light at the end of the tunnel, and she captured her patient’s narrative around depression.

She also talked about using the style of Vincent van Gogh which was her favorite artist. She talked about the heavy colors which represented how she felt after close to an hour of listening to someone who’d had a traumatic and difficult life. She even wrote some of her own experiences from her own family in the past.
You had both the patient voice coming through and the student voice in a way that you wouldn’t, in general, get in a standard written reflection on having met a patient. That’s just one tiny example, it’s so many different examples captured micro moments that would otherwise probably not have been spoken about maybe to their flatmate, but not captured in a way that I’m still talking about and showing them 10 years down the line, for example. We’re still doing new ones all the time as well, but some of those old ones are really profound.
Paula: We’ll put a link in the show notes to your website because you’ve got the collection of some of those images there. Some of them, well, I think all of them are really moving and you have that sense of just human uniqueness and diversity that as you say you can really tap into. Louise, what if a student was to come along to one of your courses, what could they expect? What would happen? What goes on?
Louise: There’s two different dimensions. There’s this small student selected component and that’s up to about 12 students. That was quite an intense, that’s like two week block where I’ll introduce them to creative enquiry, I’ll introduce them to thinking about clinical practice. I’ll also co-work with different arts for health consultants. When they come in we might have a creative writing session or a music therapy session.
The model tends to be similar for these where they hear about or they witness what patients have written, for example, in creative writing or the songs that they’ve written in palliative care. Then they hear about the process, the facilitator who holds those spaces with patients talk about how they do that. Then they have a go, they try it themselves and then they share as much as they want to of what they’ve actually created.
That’s often where the really interesting stuff happens of where they start to maybe have new ideas, see things in new ways, new horizons open for them as they hear what other people say and make their own explorations. We try to within that space, always have a time where they actually get into some creative enquiry process. That’s one of the bits that I love where a silence descends over the group and they’re creating or making something and they’re all in their own.
They go into flow I suppose, and they’re creating and making, and then we bring it back together and then share in the large group. That’s the model for the more intense two-week process. The other ways we’ve introduced it is across the whole curriculum. For example, in the GP placement, like in our GP, our year-three GP placement, instead of telling them to– teaching them on compassion, which I don’t think is that easier thing to do, we engage a head, hand and heart model that William Oslo spoke about.
That’s we invite them to think about what they’ve seen in terms of compassion and practice. They’re thinking about their lived experience of their own or what they’ve seen other people do. We invite them to investigate the literature that’s the head stuff, but also we don’t force it, but they can do engaging creative enquiry as well. This is as a group and then they present that to their GP tutors.
It’s coming from the students and I hope that in that way is more transformative and from what one of my students did research into this and found that even the GPs were being changed and learning from what the students were bringing. It’s quite nice model. We’ve had students do a musical, for example, where they’re acting out.
There’s a few musicals actually as well as poetry or group images to help explore what compassion might actually mean. We always put written reflection alongside any of the creative stuff that’s done so that it’s always bilingual. The work is always bilingual, if you like. If it’s a piece of music, there’ll be a written piece of reflection alongside it. That’s how it tends to work.
Paula: That sounds like a really fascinating process of collective creativity, must be quite an experience for students.
Louise: Then students join me to take things further. I have a student who experienced that last year and this year, wants to actually find ways to help students engage with it better because he facilitated the students in his group having worked with me previously. He’s going to do like an elective time with me, seeing how he can enable more students that haven’t really heard of this and don’t really know about it. It’s still not that well-known about across the medical school. He’s going to find ways, and I love co-creating with the students in that way because he’ll understand their perspective better than I will. Then I can bring the other dimension.
Paula: I imagine that probably much like psychologists that medical trainees, there’s a lot of perfectionism around, how do you manage that?
Louise: That’s a really– The start of that and two-week course, it’s one of the most important things I try to get across about engaging in process rather than product because that is a massive issue of not wanting to make a piece of something that looks terrible, but that obviously stops you thinking if you’re thinking about that. One of the images that I show people when I talk about what creative enquiry is by a student, I think in 2006.
She was an artist when she joined us and she’s got a picture of a girl, herself actually, with her hair covering her face.
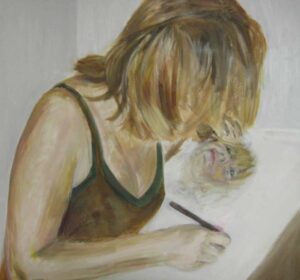
What she wrote was, “When I picked up–” She hadn’t tried creative writing before and found it transformative. She said, “When I picked up the pen and started writing, my face is emerging three dimensional from the page.” You can’t see, her hair’s covering her, but then you see this face emerging from the page to illustrate how she was connecting with herself and coming to understand herself as she wrote. The interesting thing about that image is that she was a very good artist, but actually creative writing was something she’d never tried.
It was the medium that she wasn’t necessarily so exercised in that, she wasn’t so polished in where she actually had the greater personal journey. I try to use that to explain to people, “You are going to be future doctors and clinicians, so this is about finding ways to help you to explore that. It doesn’t need to be your best, most beautiful piece.” I often use beautiful images when I’m showing it and I have to explain that, that you don’t have to be able to create this imagery. It’s just that it’s nicer to look at in a presentation, but that’s not the point really.
Paula: I saw you speak at a conference, it was just before COVID, it was the beginning of 2020 and you did a lovely exercise with the group which I’ve borrowed in different places where you had a bunch of postcards with the different images, some quite abstract, and asking the group just to pick one that resonated with them in some way and then have a small discussion in pairs or threes.
That was a really lovely exercise, and when I’ve used that it’s been really helpful because I think it enables people to access something but in a really safe way because they can choose what they’re responding to choose, how much they share or don’t share. There’s something about just accessing the symbolic and the unconscious in a way that can, as you said, get to something much more quickly than if you had a verbal discuss.
Louise: Totally. That’s been because I’ve done that exercise lots of times. I really love it. Often use it for people to just explore their lived experience, something that resonates from their lived experience. I always do the bound, like set the boundaries because sometimes something really powerful actually emerges. I invite, I say they can talk about the process rather than the actual card if it’s too personal.
At times when people feel safe, it can be very deeply meaningful. Sometimes people panic about which card to choose, but what we’ve discovered is the more relaxed you are the easier it is. Actually, because we’re meaning making creatures, probably we could make something out of any of the cards actually in the end. I use that. I often use that as a first exercise because creative enquiry can seem frightening to people and actually putting pen to paper can feel challenging, whereas picking a card is much easier.
In fact, I did a workshop back in 2006 for GPs, and one of the things that came out, they all knew each other very well. They were a trainer group. One of the things came out was quite a number of them, and they probably wouldn’t have said this if they didn’t feel as safe as they did with each other, had been told as a child that they were not good, they were terrible at drawing and that sort of thing. We had a whole day of creative enquiry and the thought filled some of them with dread.
It was good to just get that out there at the start. It’s interesting, if you’re using creative enquiry processes, we do need to be aware of the challenges in making it work. I suppose I have a model in my mind which involves things like, so if I’m doing training for people who want to do this work, it’s around having muse, getting involved yourself, setting up the boundaries and the psychological safety, using a simple exercise first before you go into something else.
Those sorts of things to enable and also to think about who we are as facilitating and how we are managing this organic space and thinking about holding transformative spaces and reading the people in the group, I think. Chris Celia has talked about the artist of the invisible when she thinks about transformative spaces. I think that’s what it is. If you’re holding those spaces, you are actually doing your own artistry in that way. There is an artistry to holding that space.
Paula: You used the word vulnerable as well and that was my sense too, a window to the soul and how it might feel for the students to be accessing that vulnerability in the setting of medical training. I suppose, I wonder partly whether using the creative process and those different mediums allows people to access that vulnerability in a oblique way, saying it, but not saying it, which creates a sense of safety. Are there also things that you’ve needed to establish in order to allow people to engage in the process?
Louise: Yes, lots of different things to say. One of the things, I’ve written a paper on vulnerable leadership as important if you’re going to facilitate these kinds of groups. These groups become a really transformative spaces. Rather than being informational learning, it’s actually a transformative. People start exploring their values, their beliefs.
They start exploring and realizing that they see the world differently to someone else. We can start thinking about becoming reflexive, not just reflecting, but actually thinking about the lenses that we are wearing when we meet our patients. These transformative spaces, they need proper holding because the students end up sharing more and more.
In fact, a couple of examples from the starter sessions, and students can feel nervous, one of the student before she shared some construction of just materials that we’d left, it’s hard for me to talk about this because you can’t create without putting something of yourself in it, and so because students are, for example in that course, whenever they’re creating, they’re putting something of themselves in it.
They’re revealing a bit more of themselves than they would in most other contexts. Another student talked about– she heard someone sharing a poem that they’d written. She’d missed the morning. I’d done lots of stuff about making it safe and talked about the process and it’s not about the product and all these things.
She came in in the afternoon and heard someone reading a poem that they’d written and thought, “There’s no way I’m going to read a poem amongst my medical colleagues. That’s just not happening.” The reason I know that is because the second week she had actually written her poem and she was then reading it and sharing it, and that’s what she told us about that. There is quite a lot of work to be done to make that space safe.
I think the vulnerable leadership idea is about giving enough of ourselves when we are facilitating those spaces to make it safe to share stuff. It’s not about us, it’s about us making space for others. For example at times, not usually at the start, but I might mention my previous experience of cancer, for example, or I might talk about challenges that I faced in practice and bring stories from clinical practice into the room.
Basically it’s around knowing that we are all human and I often say, “We’re all a bit broken. Humans are all a bit broken.” That’s the starting point. From there, we can then begin to share and explore. I think vulnerability, maybe we’ll touch on that again, but it feels to me like it’s not where we want to be but it actually is very powerful in lots of ways.
Paula: How is that received in the context of medical training? Has it been something that has been an easy time or has it been–
[laughter]
Louise: It’s been a bit of a lonely journey. I think it’s easy to misunderstand it. The students have understood it. The students who have engaged have understood it. It’s been quite a grassroots thing. I think sometimes it’s been misunderstood as like, “Oh, this is just the same as maybe going to the cinema in the evening. It’s something nice and relaxing that you can do to–” Actually for me, I started it.
For me, it’s about ways of knowing and practitioner ways of knowing and what we know and what we bring, who am I and what I bring to my encounter with patients. For me, is a fundamental part of scholarship, but it’s quite difficult to articulate and it’s quite difficult to get that into the medical journals. I have written a few book chapters and this and that, but it’s been lonely and challenging. I think the COVID pandemic has really changed.
I don’t know if it’s just that, but that feels like there’s been a sea change and there is much more openness it feels like now. In the past I wouldn’t even talk about wellbeing or flourishing, it was all focused on how we would be with patients. Even the students, I don’t think would really accept it. Now, out and out, I can talk about flourishing as well. I do a session on flourishing even though most of it has been focused on what the patients bring and do and their creative stuff in this small group one that I do.
Then I talk about the student flourishing and what’s wonderful is they explore the ideas I give them. They create around it and give things back to me so we come to understand the feel better. One of the students said, after hearing about resilience and flourishing, I’ve done a lot on trying to move beyond resilience. One of them said, “I think flourishing is a way to grow.”
Paula: I guess there’s something about that idea of flourishing really struck me because we hear a lot of stories now. I suppose I hear that a lot in my work. I do some work with trainees particularly around exam support or therapy stuff. The stories that I hear and I guess because I’m positioned in a particular way, are about how people can just survive or maybe don’t feel like they can survive anymore. It’s really refreshing to hear about flourishing, and I guess also at such an early stage in career development that people are hearing some of this stuff right at the start so that they can carry it with them. I wonder, how do you define flourishing?
Louise: That’s a great question. Flourishing isn’t much in medical education yet. I think it’s emerged because I’ve been watching in these groups that I was running, where I was trying to humanize the patient and then realize that students were being humanized and they would say things like, “I’ve learned more about myself in these last two weeks than I have in my whole 21 years.”
Or, “I can speak without censoring what I’m saying or aren’t we an amazing group of students?” Those sorts of things. It’s like, “Oh, wow, something’s going on here.” Then starting to think about this in the concept of flourishing. For the last five years I’ve been thinking exploring that. Externally I think, I realize now from the literature that flourishing is a growing concept that people are talking about more both in research and policy, but it’s not really fully conceptualized and defined yet.
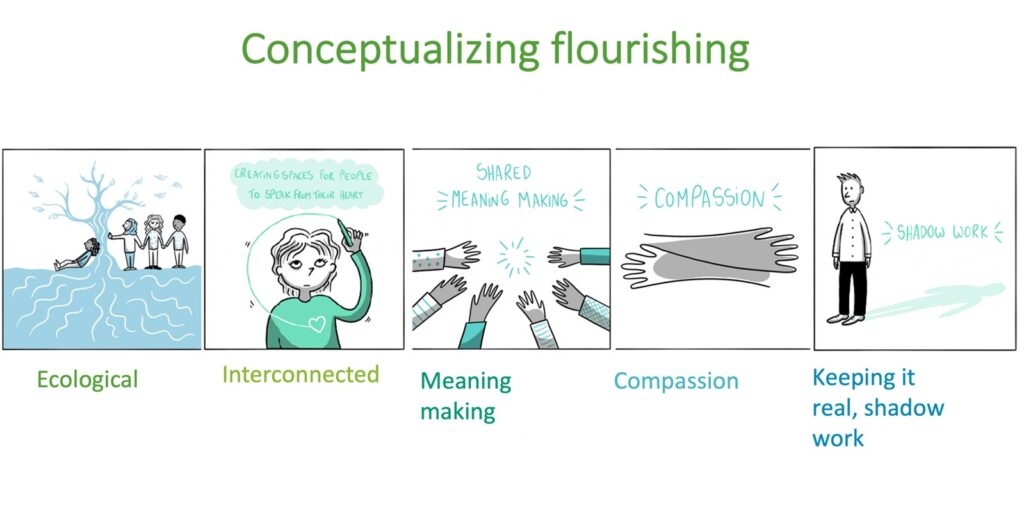
In a way I’ve got in there early. There are all sorts of flourishing models that people are bringing out. From reading a paper by Sarah Willen, she was talking about how they all have relationship and meaning making in them as part of the models as important things. They happen to be in my model as well. I’ve developed a five-block model, if you like.
I can tell you about all of those if you want, but the one thing that I have that’s perhaps different is I’ve got keeping it real or shadow work in it which I think others don’t. Sometimes flourishing can be thought of as from Aristotle’s eudaimonia. With very, very deep and long roots around meaningful and purposeful life as opposed to maybe the head-on of doing things that give you pleasure just in the moment.
Around meaning and purpose. Often it’s also thought of as everything being wonderful and excellent. Actually in my mind, for me, it’s more about being human. If we can be truer to what we are as human beings, which is a bit broken, then there’s space for us to breathe and flourish. I’ve got a keeping it real shadow work part which I don’t see in any of the other models.
That’s from observing the students. I can tell a little story about it, but young talks about shadow work and if we turn away from our shadow it gets bigger. It’s the stuff I use that to talk about the stuff that we don’t like to look at in ourselves or in our situations. For example, one of our students in a session, drew this little tiny, tiny black little fish down in a corner of an image and then loads and loads of brightly colored fish everywhere.

She described that little tiny blackfish as herself and all the others were those really bright and colorful medical students. There’s a lot of imposter syndrome and feeling compared to all the others here. Someone else did a photo with chess pieces and a little tiny grape. She said, “I felt like a grape amongst chess pieces. All the medical students honed and ready for battle.”
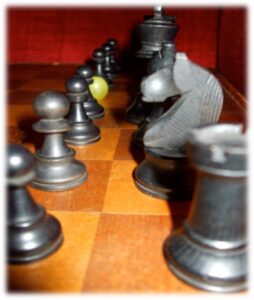
Actually at the end of this course, so this is this two weeks creative arts course, “I feel more like a grape among grapes,” because she’d heard what the other students were thinking and saying and realized that she wasn’t so different to anyone else. There’s that sense of rehumanizing, as we do the keeping it real shadow work and share some of those bits, we rehumanize ourselves and others. I’ve got five things within that flourishing which I can share or don’t need to.
Paula: Yes, please.
Louise: The first one, it’s the moving away from resilience and this idea that our inner life is something that can bounce back. Whatever traumas we go through, we bounce back to the same shape or we spring back. That idea from metals where you put more pressure on until they break and that’s how you measure how resilient they are in material science.
I don’t feel like that’s a good picture for our inner life. I often start with that flourishing is ecological. Metaphorically we think of, I’ve got a big birch tree in my garden and I look at that in season and out of season. I think of our inner lives more as something that might have seasons. We might be going through winter, but there will be a spring coming.
It allows us to think about the soil that we’ve grown on. We know, for example, adverse childhood experiences make a big difference to people’s lives. We’re not comparing one person with another. The brief resilience scores where it says, “I can bounce back from absolutely anything from 0 to 5.” These things are being given to medical students to look at, and I find them problematic because they don’t take into account where we’ve come from and what we’ve been through.
We can think about the soil, we can think about the weather that’s going on for us right now. Maybe I am feeling down hearted, but I’m actually facing a bit of a storm right now. It brings in the ecological and it feels like that’s a bit healthier in terms of thinking of our inner life as a metaphor. Then it’s interconnected, so that’s the relationship part. It’s something that is interconnected. It’s not something that I necessarily do on my own, like am I more resilient than the person next door?
Actually, I talk to them, students about the wellbeing of what is rather than the wellbeing of do something better. They get told, “Eat well, sleep well, do this, do that and then you’ll be well.” Actually, I’ve seen that when the trust is built between people, maybe through creative enquiry and the vulnerable leadership, they share a bit more. They realize they’re not alone. They might talk about the exams that they’re worried about, whatever it is, and they actually feel better.
There’s a sense of feeling better, even though we haven’t changed, they haven’t had to do something different. There’s something about if you just increase the trust between those connections, I guess it’s systems thinking. If you enhance the connections between, or catalyze the question, the connections between people, there’s a sense of flourishing emerging. Then there’s a meaning making, and I’ve already spoken about Aristotle, and I often show that image that I described of the woman slumped over in the van Gogh style.
There’s a sense of the patient voice and the student voice, for example, that you get this deeper meaning making through the creative enquiry that leads to flourishing. Then there’s compassion, which can be compassion for self or compassion for others. Students often have that sense that they can’t be compassionate towards themselves. One of the students did a beautiful image with the faces that you put on to the world and newspaper hands with zigzag hands, with strings holding those faces.

It’s a great image, and then she has underneath a kind hand with a ball of wool and just saying, “We can choose to be kind to ourselves.” As a result of, I think, other things going on as well as the course, she talked about, “I can actually make time for my friends. I can actually make time to crochet. I don’t have to be the best always and it is okay to make mistakes and then to come back.” There’s something around compassion and building that in and how that can lead to flourishing. Again, it’s the humanizing and the final one is the shadow work and keeping it real.
Paula: It strikes me as a beautiful model that allows the individual and the systemic to come together. I think there’s often a tension there where we face the causes of burnout, for example, are these really big, huge problems that we as little people can’t fix, which can feel like a very hopeless place to be.
Then on the other hand, you might get this kind of resilience move that the problem is located within you and you just need to be bouncier, which is also very problematic. I guess, I love what you’ve drawn out there in terms of being able to keep it real and connect with our worlds, our people, our ourselves and our humanness. Holding that all together is really powerful.
Louise: Yes, I guess I’m testing it out all the time by sharing it and seeing how it lands. Does it land well? It does seem actually for students and clinicians to land and bring a sense of relief somehow, I think.
Paula: One of the other things that struck me was that sense of humanizing us as health professionals. I think that’s one of the things that I often hear about the people working in therapy with is that sense of being stripped of their humanity, either through the ways that systems work in terms of people just feeling like they’re a nameless rotor feeling function, or just not having basic human needs met in terms of being able to go to the toilet or get food.
Louise: I remember it. [laughs]
Paula: Then also the other part of how brutal it can be to continually face suffering, to not be able to meet patients’ needs because of, whatever, lack of resources, and to have no recognition of that in the system, especially over a long time, can be a really dehumanizing experience. I think creativity can be a really important way back to that.
Louise: I think about my own practice, and I am now working not many sessions as a GP, and I don’t run to time, [laughs] but the system does push us to practice in a certain way. I sometimes say to the students, “Only dead fish go with the flow.” If we don’t go with the flow and actually, I think we forget that bringing ourselves actually and deep listening, we can’t solve all of our patients’ problems, but we can hear them, and we can be present and we can witness them.
We can also do some stuff, that’s great when we can do stuff, but some of the time we can’t, and I think we forget or because it’s so trained out of us and we’re so blinkered, we forget that actually the power of being there and being present. I guess I’m increasingly interested in trauma and trauma informed care and people are coming and sharing things with me. I can’t take it away, but deep listening and presence and helping people to make start, to make sense of things can be part of a healing journey.
I suppose part of what I love about practice when it happens is when I’m still learning, and every person, every patient, when there’s opportunity– and that is hard in the system. I guess, [chuckles] I make a choice to take a bit of extra time to have those more meaningful conversations. Even if you just have one of those, I think that that can really help you fall back in love with being a clinician and the privilege of meeting people at a point that is raw and vulnerable.
Even it really, so before my cancer which was in 2014, I felt like I’d learnt so much, being a GP for about 14 years, I’d learn so much from my patients that did help me going through those times. I suppose I’m saying that because we are human too, we are not beyond diseases and illnesses and in a sense we are two people on a journey trying to do something good in that moment.
Paula: I’m wondering if that’s part of– You mentioned about COVID being part of a shift. I was thinking when you said that, whether a part of that is those two coming together, the vulnerability of doctors, nurses, people on the front line, in a way that we couldn’t ignore anymore.
Louise: Yes, there’s a great article. I just love the words I keep quoting, it says, “COVID grief has cracked us open.” The clinicians, and I think there’s a truth in that, isn’t there? Not that I want people to be cracked open. One of the things I’d really like to do in the long-term is, often the human dimension of medicine is called the soft stuff, i.e., the soft easy kind of.
Just even the language we use, sort of down regulates the importance of it and how profound it can be in people’s lives if we engage with it well. I’ve got an image with two strands of the DNA and one is the clinical dimension, which is well articulated in medical education. The other is the human dimension and I believe it would be possible.
I think even Engel who developed the biopsychosocial model in one of his articles, said, “The human dimension is possible to articulate.” It might be challenging, it might not fit into our models, but it might be more about making spaces rather than telling people stuff or examining them on stuff. I think it’s possible.
Paula: I think it’s probably essential like some of these bigger issues that we’re struggling with right now in terms of the workforce and recruitment and retention. I think in all the conversations there’s very little that you hear at the policy level about the human dimension, which is the reason why people leave. It’s those very human things, needs that can’t be met. I think we need to keep it real, don’t we? Grapple with those things if anything’s going to change.
Louise: Yes, I think so. There’s a lot of talk about trying to get the doctors to offer person-centered care and have that. Actually, the understanding of that, there’s a great paper published in December by Aarti Bansal and team. They just showed it isn’t enough in our positivist curriculum where we’re teaching knowledge and skills and facts as if forgetting all the intersubjectivity of what happens. It isn’t enough just to do some communication skills training.
Well, what they found from their research was you need space for emotions, you need space for the patient voice, you need space for meaning making. If we are going to help doctors in the future, be able to do any person-centered care. There’s a lot of talk about person-centered care, but actually, how do you filter down to enable that? It isn’t through just telling doctors to do it, we’ve got to walk the walk within the education process, I think.
Paula: If you could wave a magic wand, what would you like to see happening in our healthcare systems beyond the undergraduate education bit in terms of creative enquiry and–
Louise: Well, also trustee of various of Arts and Health South West and I’m co-chair of the Royal Society of General Practitioners Arts and Health group, and I also had a poet and an artist in my surgery for three years as also something that I really wanted to do for my patients while we had the funding. It was amazing.
It was so wonderful to hear their stories, to see people building friendships, to see there’s a lot of loneliness out there, so to help people to come together. They weren’t really talking about their diseases, they were just being rehumanized I suppose. I haven’t thought about it in that way, but they were sharing their stories and their lives through the arts or through poetry and finding new ways and new friends.
I’m not saying that arts solve everything for sure, but I would love there to be some arts-based practice in every GP surgery for example, that we could refer to, that they would access, because so many of the problems we see, a lot of the chronic pain and all sorts of things that we’re seeing, a lot of stuff is result of trauma and pain and other things. There’s no space to give voice to any of that. In a 10 minute consultation, there isn’t any space, so people just bounce around being given drugs, being given this and that.
That might be part of it, [chuckles] a proper– obviously we’re seeing more impact of– this is way beyond the scope where we’re seeing more impact from the inequity, and so a proper leveling up because that starts to impact our patients and the people that we see as they experience more and more challenges. I suppose that’s the fundamental level in a way at the starting point. There is evidence as well for the arts-based processes. It’s just a bit harder to measure and manage in the monetary system that we have in a way.
Paula: For anybody who might be listening to this and and be really excited about the idea of creative enquiry and how those process of creative expression can support us in this work, any thoughts about how people could take some of these ideas and put them into action without having access to one of your wonderful courses, either as individuals or in teams?
Louise: There’s some of it, I wonder it might be the underpinning thinking. I’ve got three Vs in terms of the underpinning thinking which I’ll share and then maybe we can just think about what that might mean in practice. This is from a book chapter I was writing and it feels like these three things are really important to us to flourish. One of them is vulnerability. Actually as an individual, being able to recognize that we are vulnerable, then we don’t have to fight it at least.
Being able to find spaces where we can be vulnerable, is powerful even if it’s one other person where we can be real. There’s something about finding our voice, so the uniqueness of what it is that I bring into the world and how I see the world. For that to be heard as well, again, I think can profoundly lead to flourishing. The third one is valuing humanity, so that recognition that we are a bit broken and being kind to ourselves in our humanity, rather than judgmental on ourselves or others.
Those three things, I think, are core and underpinning to flourishing different ways that we might– As an individual I think, or what I’ve read and heard from the students that making space and time to see friends, to value those spaces, it’s not all about either trying to achieve things or to make money or whatever, that actually you value a space for being. Whether that’s crocheting, or cooking, or baking, or I don’t know, cycling or whatever, walking in nature. You have to value that.
It’s one of my students said in her second year at medical school, “I stopped painting when I came to medical school and it’s not because I didn’t have time, it’s because I stopped valuing it in the system.” After the creative art school, she said, “Now I’m going to paint anyway for me because I want to.” It’s that sort thing. She’s still painting [laughs] about 10, 20 years down the line. There’s something about creativity, valuing that space, being aware of our vulnerability and trying to find spaces where we can give voice to what it is we see.
In teams, essentially I’ve been invited into a GP practice and that will be a new venture for me, so to work across the team there, to think about how we explore flourishing within the team. I think if we were to think of those three things again, is this a space where people are able to express their vulnerability without being hammered to actually be real? Is it a space where people can actually give voice to some of the stuff that they see, and feel, and hear?
Are we valuing our humanity recognizing that we need space for breaks, we need to support each other, and so building those links between us. It’d be interesting to see, we’re going to do some creative enquiry work that will be facilitator stuff and then they’ll also do some other stuff. I think it starts with actually recognizing that we are a human team and how we find that. In terms of organizations, I’m a flourishing fellow as well at Queen Mary University of London where I’m working.
Paula: It’s a nice title.
Louise: It’s a lovely title, isn’t it? I love it. Flourishing fellow. Part of that, their highest mission is that their students and staff will flourish.
The question is and part of their goal is to be– we’re in East London, so is to be an inclusive university with widening participation. What does that mean and how does that look as an organization? I think still those three things that the value and humanity vulnerability and voice impact, but that’s, I think, work in progress. That’s beyond where I’m exploring these things.
Paula: Thank you for listening. If you enjoy this episode and you’d like to help support the podcast, please do share it with others, post about it on social media or leave a rating and review. I’d love to connect with you, so do come and find me on LinkedIn or Twitter. You can also sign up to my mailing list to keep up to date with future episodes and get useful psychology advice and tips straight to your box. All the links are in the show notes. Thanks again, and until next time, take good care.